Why is my shoulder hurting? What your doctor may have overlooked!

Is your shoulder giving you problems? Have you tried seeking treatment for your shoulder to no avail? Are you sick and tired of dealing with that constant nagging ache? Maybe you thought you’re getting older, and your shoulder will never feel fully healthy again. It’s time to take a second look at that shoulder and what may be causing your pain!
The prevalence of shoulder pain in the general population is estimated to be 15.4% in woman 24.9% in men according to a recent epidemiology study (Pribicevic, 2012). Injuries and dysfunction of the shoulder falls into four categories; fractures, joint injuries, muscular injuries, and functional imbalances. Fortunately the first three categories are easily identified with orthopedic testing, x-rays, MRIs, and most often can be successfully managed. The problem is that when you fall into the fourth category, functional imbalances, you shoulder problem can be easily overlooked. The medical community at large has focused mostly on pathologies of the shoulder and less on imbalances. It is these functional imbalances of the shoulder that can plague a lot of us, sending us in circles from one treating provider to another with no help. It’s time to understand what is going on!
Let me first start by giving you a brief anatomy lesson of the shoulder region. The shoulder is comprised of three bones, the humerus, scapula, and clavicle. The humerus, the upper arm, fits like a ball and socket into our scapula aka shoulder blade. This is called the glenohumeral joint. The scapula connects to our backs and forms the scapulothoracic joint. The clavicle, aka collarbone, connects to the scapula at the acromion, a bony process that extends outward from the scapula. This union between the acromion and clavicle forms the acromioclavicular joint, better known as the AC joint. At the other end of the clavicle is the sternum, aka breast bone. This makes up the bones and joints of the shoulder. Then you have your rotator cuff muscles that provide stability and mobility to upper arm at the glenohumeral joint. The glenohumeral joint, has more mobility that any other joint in our body.


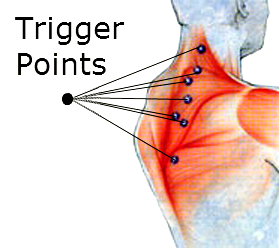
Surprisingly, most shoulder functional imbalances are not located at the shoulder but the muscles surrounding the shoulder. Commonly people have what is known as upper cross syndrome. The shoulders that are rolled inward, a head that protrudes forward, and a rounded back. It’s no surprise with today’s culture of tablets, cell phones, and increase work at a desk, we are seeing a rise in the prevalence and early onset of this functional imbalance. When you carry your body this way, you chest muscles, the pectoral muscles, become contracted pulling the shoulders forward and inward. You muscles in the front portion of your neck become inactive and your head slumps forward. You actually decrease your lungs capacity and the ability for you to breath deeply. Your back muscles, rhomboids and serratus anterior, which are responsible for holding the scapula firmly against the back turn off. The traps and levator scapula become tight, and the scapulae migrate up, outward, and internally rotate. This is what we call an anterior tilted, lateral translated, internally rotated scapula. This is functional imbalance of the shoulder, it’s a problem, and many of you reading this are experiencing this to some degree now.

The joints of the shoulder, the glenohumeral and acromioclavicular are now wearing at each other. The space under the acromion has become diminished and inflammatory processes, swelling, and degeneration start to set in. Left uncorrected the degenerative changes continue to erode at the shoulder and rotator cuff repairs, acromioplasty, and shoulder arthroscopy may become common procedures for some. Most of this can be avoided if the problem is address early and restorative measures and begun to return the shoulder and body back to balance. Corrective exercises, stretches, adjustments, and myofascial release can reduce and correct these functional imbalances. Having a knowledgeable physician, doctor, or therapist familiar with treating functional imbalances is key when choosing a provider. We are especially good at identifying and correcting functional imbalances of the whole body at our chiropractic office here in Jacksonville, Florida. It’s what we do.
Some great first steps to take if you suspect you may be suffering from upper cross syndrome is start some corrective exercises. You can see some being demonstrated here; https://youtu.be/7l2TLBkFnP0. If you feeling extra charged up, you can also try these scapula mobility exercises done here; https://youtu.be/hzozw2Aso3M. Doing these will help not only help you stand up taller, but also reposition the scapula and shoulder, reducing the functional imbalance and providing some much needed relief.
Remember there are many conditions that can affect the shoulder, but in summary, if neither of the first 3 categories are an issue, you fall into the fourth category of functional imbalance. Please see someone familiar with treating these type of issues and at minimum start trying some of the exercises I have linked above. There are may other videos on YouTube you may find useful for correcting functional imbalances of shoulder and body. Kelly Starrett’s channel is a great place to start. I hope you enjoyed learning about the shoulder and remember to enjoy the day!
-Dr. Colt Andrea D.C.
Mario Pribicevic (2012). The Epidemiology of Shoulder Pain: A Narrative Review of the Literature, Pain in Perspective, Dr. Subhamay Ghosh (Ed.), ISBN: 978-953-51-0807-8, InTech, DOI: 10.5772/52931.