Why do I have a disc herniation, and now what?

Having a disc herniate, bulge, slip or rupture can be a very trying time for the person experiencing it. There is a lot of information out there about what causes disc pathology and what to do when experiencing these issues, some of it good and some bad. I have treated hundreds of people with disc herniations with great results and what I can tell you is that there is no one cookie cutter approach for everybody; it takes a careful examination, appropriate therapeutic modalities, rehabilitation, and time to ensure a successful, long-lasting path to recovery.
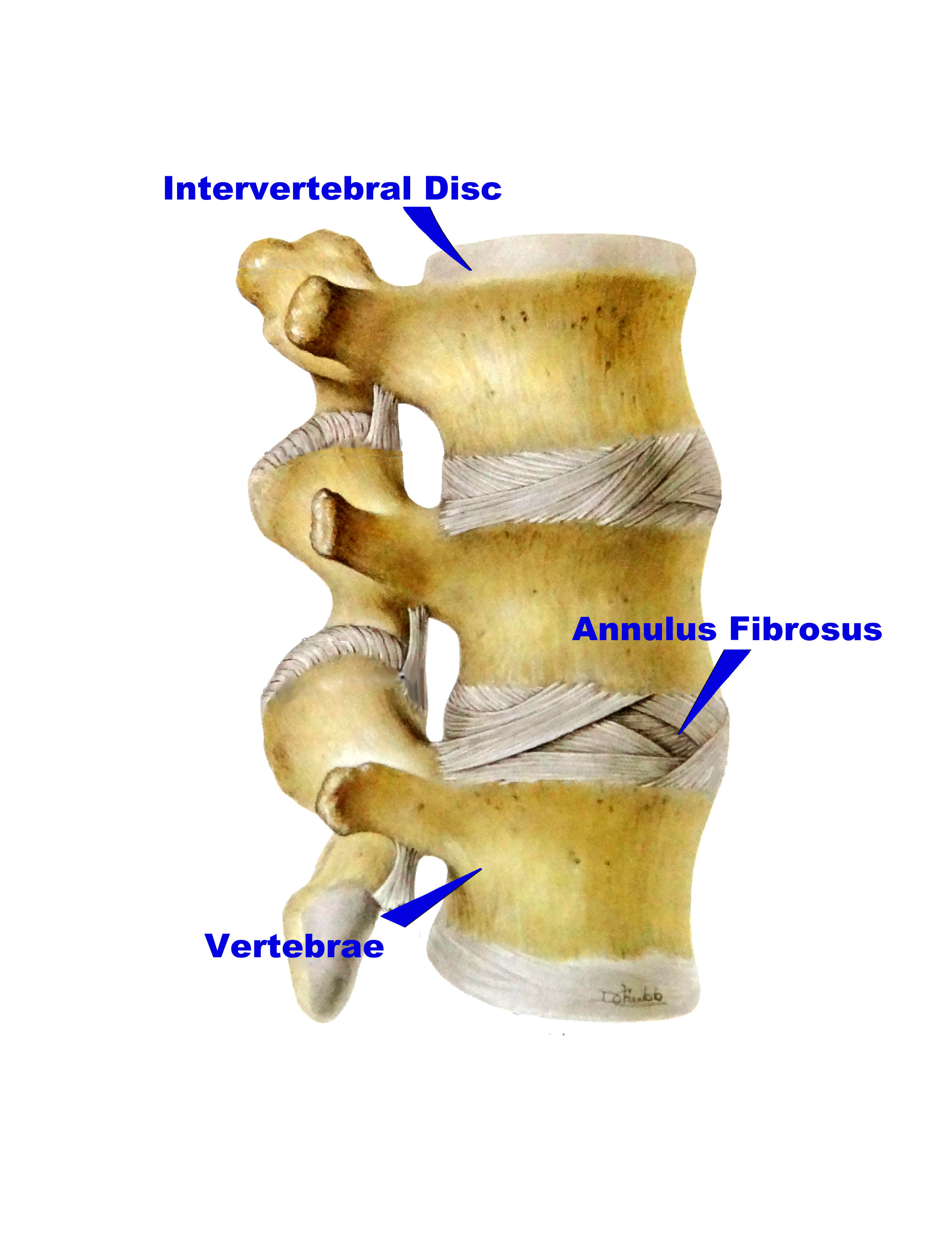
Why does the disc herniate in the first place? The anatomy of your disc, also known as the intervertebral disc, gives us clues to this. The disc, located between the vertebrae of the spine, acts very similar to a supporting load bearing cushion for our spine. Lots of people are familiar with the analogy of the jelly doughnut, and that when a disc ruptures it’s like the jelly of the doughnut squeezing out – which is a great, simple, and fast explanation to use in office. More correctly though the disc is comprised of many concentric ligamentous fibers known as the annulus fibrosus. These ligamentous fibers run at opposing angles to each other in multiple layers to make a very strong and resistant ligaments exterior boundary that contains the nucleus pulposus. The nucleus pulposus would be the jelly from our example earlier and the annulus fibrosus is the doughnut that encases the jelly, so to speak. The nucleus pulposus is composed of a loose network of collagen fibers and water that make it elastic and jelly-like, able to evenly distribute the forces and pressures applied to the disc from everyday life.
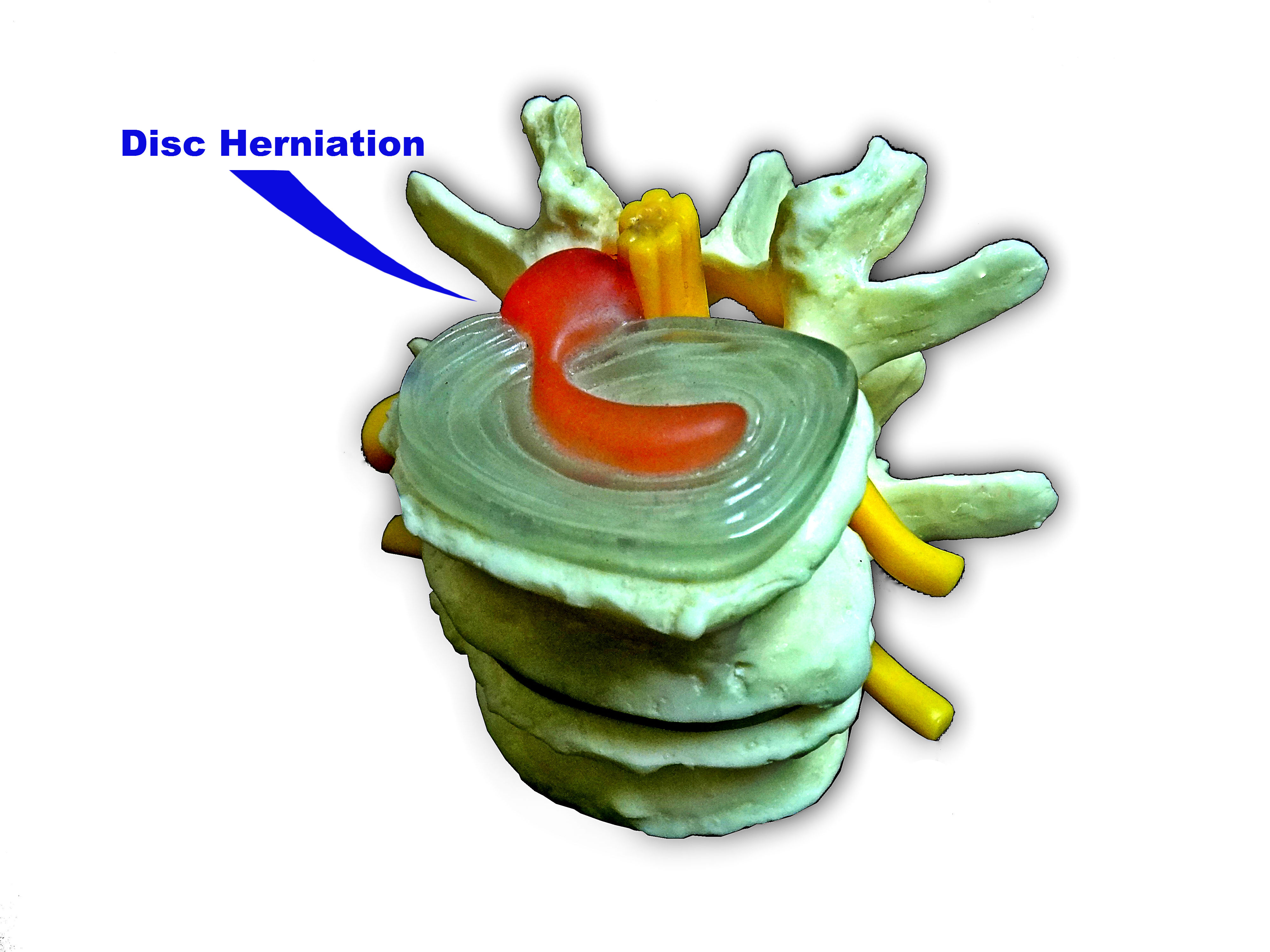
So where does it go wrong? The annulus fibrosus, these concentric, layered, opposing fibers, are very strong when force is applied in a manner that they were designed to handle the stress; but with any good design, improper use can and will lead to failure. This means improper lifting, repetitive flexing and twisting, overuse, dehydration, prolonged sitting or driving, a sedentary lifestyle, and of course, injury can cause failure. The annulus fibrosus begin to tear and separate between the fibers and layers. It may be something like a little back pain here, a sore ache another time or a noticeable full on episode of swelling, deep, achy, sharp, I-need-a-day-off-from-work type of pain. These microscopic tears create opening, and over time, with multiple episodes of tearing and separation of the layers and fibers, the nucleus pulposus is finally at a point where is has channeled through these multiple tears and fissures of annulus fibrosus that you are left with only one or few supporting layers left! This can take years to happen and is most common in our 30’s to 50’s. Finally, you drop your razor in the morning or sneeze during the day and that last layer of the annulus fibrosus lets loose and the contents of the disc, the nucleus pulposus, spill out of the disc under pressure and into the spinal cord canal where a cascade of biological events happen leaving you with a great deal of pain, swelling, and inflammation. This is also a common cause of sciatica due to the close proximity of the spinal nerve roots to the disc.
This is the point where it may be confusing for some: your back is fine and suddenly goes out while performing a simple, ordinary task that has not been an issue for you in the past, but hopefully, now you can understand and see how all previous events of back pain, bending at the waist, and a sedentary lifestyle have added up and accumulated to cause the perfect storm. Life may come to a screeching halt at this point as it’s very hard to do anything when your “back is out!” This is a very unhappy place to be right now, but rest assured there is a way to get your feet back under you and a light at the end of the tunnel.
Chiropractic care has been demonstrated to be a safe and effective means of treating and disc herniations. Gentle spinal adjustments can be done to help increase joint mobility, improve physical function, and relieve joint pain. Passive care such as ice, ultrasound, and electrical muscle stimulation may also be used to modulate pain, reduce swelling, and relax the surrounding muscles and tissues. After the initial phase of acute pain and swelling it may be appropriate to move from passive therapies to more active physical therapies such as active rehab focused around core development and strength with progression to encourage more favorable long term outcomes. At times adjunct therapies such as spinal decompression may be used in cases where progression has stalled or is slower than we would like, each case is different and is treated uniquely in our office. At times, it may be necessary to see a physician specializing in pain management for epidural steroid injections to help manage pain and swelling. In most cases this is not necessary, but can be very beneficial. With time, proper care, and the knowledge you will learn here at our office, your disc will heal and you will be back to the activities you like with the tools necessary to maintain a strong and healthy back!
-Dr. Colt Andrea, D.C.
